SKIN SWELLINGS AND NAEVI

Swellings and naevi are commonplace. Most of us seem to have multiple ones and many are used as personal identification marks. These can be present from birth or acquired later. Most of these swellings are benign. They are usually removed for cosmetic reasons or biopsied to ascertain a diagnosis. In some cases they can affect the function, for example, a swelling arising in close proximity to the eyes can impair the field of vision.
Most of these swellings in adults are removed under local anesthesia as an outpatient procedure. The excision margins are marked with a small margin and the wound edges are closed primarily. The patient returns for suture removal, which is done between 4 to 7 days. The scar is usually taped for 2 weeks for optimal outcomes.
Usually, the resultant scar is a thin line. Scar management techniques help in obtaining good scars in case the patient has a tendency for hypertrophic scarring.
In small children, general anesthesia is usually indicated. It is a safe procedure and children can be discharged the same day. In case, the tissue is biopsied the results are obtained within a week. Further treatment is based on the biopsy report.
Other complications like infection and delayed healing are extremely rare.
Different techniques for removal of benign lesions include:
1. Serial excision: In this a large area is tackled by removing the affected area under stages. A part of the affected lesion is removed and the wound edges are approximated. Rest of the swelling is removed later allowing time for normal skin around the lesion to expand. This is technique is commonly applied for post-burn scars and broad naevi.
2. Purse string closure: This may be employed in a situation where one wants to limit the length of a scar either because the length is cosmetically unacceptable or else due hypertrophic scarring tendencies of an individual.
The resulting defect after removal of the lesion is closed as a purse string. This results in folds of skin radiating from the suture line which slowly subside during 3 to 4 months. Further, a touch-up procedure may be needed to improve the appearance of the scar in some cases.
3. Full thickness skin grafts (FTSG) : This is employed in areas where a primary approximation may be difficult. This is most commonly employed in eyelids, forehead and lower part of the nose. The donor sites of FTSG are the area behind the ears, upper eyelid and flexion creases of limbs. This is selected based on the tissue properties of the recipient site.
4. Local flaps: These are used when there is a defect with resultant exposure of structures like cartilages or bone. Sometimes they are indicated to minimize the secondary contraction after the procedure. This is important for areas around orifices. Flaps have the advantage that they closely mimic the texture and pigmentation of the area that it substitutes.
Most of these swellings in adults are removed under local anesthesia as an outpatient procedure. The excision margins are marked with a small margin and the wound edges are closed primarily. The patient returns for suture removal, which is done between 4 to 7 days. The scar is usually taped for 2 weeks for optimal outcomes.
Usually, the resultant scar is a thin line. Scar management techniques help in obtaining good scars in case the patient has a tendency for hypertrophic scarring.
In small children, general anesthesia is usually indicated. It is a safe procedure and children can be discharged the same day. In case, the tissue is biopsied the results are obtained within a week. Further treatment is based on the biopsy report.
Other complications like infection and delayed healing are extremely rare.
Different techniques for removal of benign lesions include:
1. Serial excision: In this a large area is tackled by removing the affected area under stages. A part of the affected lesion is removed and the wound edges are approximated. Rest of the swelling is removed later allowing time for normal skin around the lesion to expand. This is technique is commonly applied for post-burn scars and broad naevi.
2. Purse string closure: This may be employed in a situation where one wants to limit the length of a scar either because the length is cosmetically unacceptable or else due hypertrophic scarring tendencies of an individual.
The resulting defect after removal of the lesion is closed as a purse string. This results in folds of skin radiating from the suture line which slowly subside during 3 to 4 months. Further, a touch-up procedure may be needed to improve the appearance of the scar in some cases.
3. Full thickness skin grafts (FTSG) : This is employed in areas where a primary approximation may be difficult. This is most commonly employed in eyelids, forehead and lower part of the nose. The donor sites of FTSG are the area behind the ears, upper eyelid and flexion creases of limbs. This is selected based on the tissue properties of the recipient site.
4. Local flaps: These are used when there is a defect with resultant exposure of structures like cartilages or bone. Sometimes they are indicated to minimize the secondary contraction after the procedure. This is important for areas around orifices. Flaps have the advantage that they closely mimic the texture and pigmentation of the area that it substitutes.

Mole in the left cheek.
|

Barely visible scar after removal.
|

Mole of the forehead
|

The resulting defect covered with a local flap to minimize eyebrow distortion
|

A black mole (naevus) in alar crease
|

Excision and coverage with a local flap to minimize tissue distortion
|

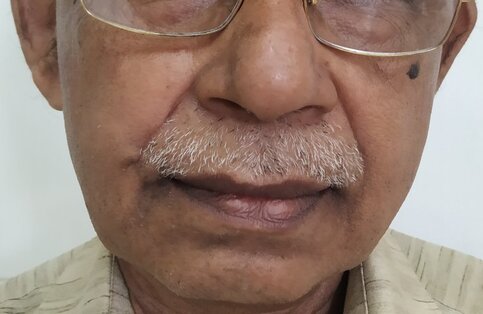
A black mole of right cheek.
|

Mole removal done with linear closure of the wound.
|

Lipoma of forearm
|

Lipoma removed by liposuction and avulsion with a small incision
|

Before: Swelling of the nasolabial region in an elderly person
|
After: 2 months postoperative appearance
|

