BREAST AUGMENTATION

Small breasts can result in low self-esteem and impaired self-confidence. This can affect the quality of life of the affected individual. Cosmetic surgery for enhancement of the appearance of breasts is one of the most commonly performed procedures. Millions of women have undergone breast augmentation resulting in a positive body image and improved self-confidence.
Small breasts are seen in the settings of:
1. Developmental: It can occur as an isolated abnormality or may be associated with abnormality of the chest wall.
2. Involutional: This is seen due to changes in the postpartum (after childbirth) period. It can be exacerbated by significant weight loss.
What are the benefits of breast augmentation?
1. Improvement of volume (size) and projection of breasts
2. Improved aesthetics
3. Improved self-confidence
Type of breast implants:
1. Silicone implants: Silicone implants consist of a shell filled with silicone gel. These do not deflate even after rupture of the surrounding shell. After breast implants with a silicone implant individuals must follow up regularly to check the status of the implants. Silicone implants have been found to be safe after years of research and are not associated with diseases elsewhere in the body.
2. Saline implants: These consist of a implants filled with saline. They deflate in the case of a leak and saline is absorbed by the body.
3. Round breast implants: Because they are round, these lead to better fullness in the upper part. There are not associated with deformity due to a rotation. High profile implants help achieve better projection for a given volume.
4. Textured implants: These allow scar tissue to stick to the implants. These are associated with reduced chances of contraction of scar capsule around the implant.
Other option for breast augmentation: A Fat transfer is a plastic surgery procedure in which fat is transferred from thighs and abdomen to the breast. It is undertaken for women who want a small increase in the breast volume.
Who is a good candidate for breast augmentation?
1. Those in good health and nonsmokers.
2. The absence of concomitant ( co-existing) breast diseases. A screening mammogram is advised for those above 40 years of age.
3. Individuals dissatisfied with the small size of breasts.
4. Those with realistic expectations.
How to choose an implant that is right for you?
Choosing an implant shape and size is undertaken jointly by the individual and plastic surgeon. In order to optimize the appearance various parameters like size of chest, breast diameter, breast height and skinfold thickness and stretch-ability of the skin envelope are seen. For improved projection for a given size (in ml) can be obtained with the help of high profile implants.
Procedure and recovery:
Breast augmentation is carried out as a short stay or outpatient procedure. Patients are started on a course of antibiotic pre-operatively. The procedure is carried out under general anesthesia. The implants are usually placed through a small incision on the undersurface of the breast. A pocket is created either behind the chest muscle or the breast tissue. The wound is closed with sutures. Postoperatively an individual is put on pain medications. Dressing is used which help in minimizing implant displacement. Stretching exercises are begun in the postoperative period to minimize the occurrence of capsular contracture. Light work can be resumed at the end of the first week. Patients should refrain from heavy exertion till the end of 3 weeks.
Correction of primary hypomastia:
It is the impaired development of the breast tissue. Sometimes it can be associated with anomalies of the chest wall. In the case of unilateral hypomastia treatment is begun when there is no further increase of breast tissue with age.
Because the overlying skin and soft tissue are tight a pocket is first created with the help of a tissue expander. This is a device which can be progressively distended with the injection of saline. This is carried out at weekly intervals till the size matches the contralateral normal breast. The expander is later exchanged for a breast implant after the breast develops ptosis. The goals of treatment of primary unilateral hypomastia are to increase the fullness and projection of the breast while matching the appearance of the unaffected breast.
Small breasts are seen in the settings of:
1. Developmental: It can occur as an isolated abnormality or may be associated with abnormality of the chest wall.
2. Involutional: This is seen due to changes in the postpartum (after childbirth) period. It can be exacerbated by significant weight loss.
What are the benefits of breast augmentation?
1. Improvement of volume (size) and projection of breasts
2. Improved aesthetics
3. Improved self-confidence
Type of breast implants:
1. Silicone implants: Silicone implants consist of a shell filled with silicone gel. These do not deflate even after rupture of the surrounding shell. After breast implants with a silicone implant individuals must follow up regularly to check the status of the implants. Silicone implants have been found to be safe after years of research and are not associated with diseases elsewhere in the body.
2. Saline implants: These consist of a implants filled with saline. They deflate in the case of a leak and saline is absorbed by the body.
3. Round breast implants: Because they are round, these lead to better fullness in the upper part. There are not associated with deformity due to a rotation. High profile implants help achieve better projection for a given volume.
4. Textured implants: These allow scar tissue to stick to the implants. These are associated with reduced chances of contraction of scar capsule around the implant.
Other option for breast augmentation: A Fat transfer is a plastic surgery procedure in which fat is transferred from thighs and abdomen to the breast. It is undertaken for women who want a small increase in the breast volume.
Who is a good candidate for breast augmentation?
1. Those in good health and nonsmokers.
2. The absence of concomitant ( co-existing) breast diseases. A screening mammogram is advised for those above 40 years of age.
3. Individuals dissatisfied with the small size of breasts.
4. Those with realistic expectations.
How to choose an implant that is right for you?
Choosing an implant shape and size is undertaken jointly by the individual and plastic surgeon. In order to optimize the appearance various parameters like size of chest, breast diameter, breast height and skinfold thickness and stretch-ability of the skin envelope are seen. For improved projection for a given size (in ml) can be obtained with the help of high profile implants.
Procedure and recovery:
Breast augmentation is carried out as a short stay or outpatient procedure. Patients are started on a course of antibiotic pre-operatively. The procedure is carried out under general anesthesia. The implants are usually placed through a small incision on the undersurface of the breast. A pocket is created either behind the chest muscle or the breast tissue. The wound is closed with sutures. Postoperatively an individual is put on pain medications. Dressing is used which help in minimizing implant displacement. Stretching exercises are begun in the postoperative period to minimize the occurrence of capsular contracture. Light work can be resumed at the end of the first week. Patients should refrain from heavy exertion till the end of 3 weeks.
Correction of primary hypomastia:
It is the impaired development of the breast tissue. Sometimes it can be associated with anomalies of the chest wall. In the case of unilateral hypomastia treatment is begun when there is no further increase of breast tissue with age.
Because the overlying skin and soft tissue are tight a pocket is first created with the help of a tissue expander. This is a device which can be progressively distended with the injection of saline. This is carried out at weekly intervals till the size matches the contralateral normal breast. The expander is later exchanged for a breast implant after the breast develops ptosis. The goals of treatment of primary unilateral hypomastia are to increase the fullness and projection of the breast while matching the appearance of the unaffected breast.
Related topics:
1. Myths surrounding breast augmentation
2. Breast augmentation as part of sex reassignment surgery (SRS)
1. Myths surrounding breast augmentation
2. Breast augmentation as part of sex reassignment surgery (SRS)
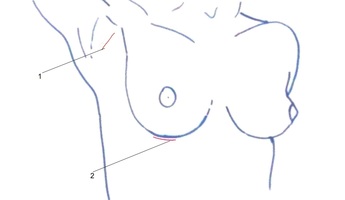
Breast augmentation incisions: 1. Axillary (arm-pit) 2. Infra-mammary (along the lower fold of breast)

Asymmetric breasts in a 39 year old
|

Breast augmentation with 360 ml moderate profile implants in submammary plane
|

Before breast implant undertaken as part of SRS
|

After sub-mammary silicone breast implants
|

Hypomastia of the right breast
|

After first stage correction with subpectoral tissue expander
|

