BREAST REDUCTION

Reduction mammaplasty or breast reduction removes excess skin, fat and glandular tissue from breasts to make it proportionate to rest of body. Patients with excessively large breasts can be affected due to the physical effects of large breasts. It can also result in embarrassment which may prevent an active social life.
Am I a right candidate for breast surgery?
You are a good candidate if,
Breast reduction surgery can be performed at any age. It is, however, best performed after the breasts have matured. Breast reduction surgery can impair the ability to lactate ( breastfeed ). In case you are planning a future pregnancy, this must be brought to attention. The results of breast reduction can be affected by any future weight changes and pregnancy.
What are the steps involved in undergoing breast reduction surgery?
These are:
Preoperative consultation. You should be able to discuss your goals and expectations. We will be able to possible outcomes based on the physical examination findings. You must be prepared to the reveal history of any coexisting medical illness, medications, herbal supplements, any prior breast surgery. The incisions and scars location will be shown to you. The risks and possible complications are discussed. A mammogram is usually taken and depending on the findings further investigations like ultrasound may be ordered. Medical tests for fitness to undergo the procedure are obtained. Preoperative pictures are taken. You should feel free to clarify your doubts about the procedure.
Procedure. Breast reduction is usually carried out under general anesthesia. The incisions depend on the physical examination findings. They are usually,
The incisions are deepened after removal of excess skin. The breast tissues are reshaped and excess tissue is removed. Sutures are placed to hold the breast tissue together and incisions are closed with sutures and tapes. There may be thin tubes placed which help prevent accumulation of fluids at the operated site. Dressings comprise of soft pads placed in a surgical bra.
Recovery. Patients are encouraged to move about when they recover from anesthesia. The dressings are removed during the second day after surgery. The drains are removed depending upon the output. Patients are advised to cover the suture lines with dressing till suture removal. Most sutures are removed by the end of the first week and rest are removed at the end of the second week. A support bra has to be worn till three months. Light activities are permitted after the first week. Overhead movements of arms are restricted till the end of three weeks. It is usual to have swelling and some bruising at the operated site. These gradually resolve with time. Some patients may have numbness of skin near the scar. In most cases these settle without any intervention.
Will breast reduction impair the ability to lactate?
Yes, it can.
Will it affect imaging studies after surgery?
Yes. It can result in changes which can affect the interpretation of imaging studies on the breast.
What are the benefits of undergoing breast reduction?
These include,
To learn more about secondary breast reduction, click here.
Am I a right candidate for breast surgery?
You are a good candidate if,
- You are bothered by the excessive size of breasts.
- You have back ache and difficulty in working out as a result of large breasts.
- You get indentation on the skin due to the bra straps.
- There is maceration of skin in the folds on the under surface of breasts.
- There is inferior displacement of the nipple.
- There is a widening of the areola due to stretching.
- You are in good health without any significant co-existing illnesses.
- You do not smoke.
- You have reasonable expectations about breast reduction surgery.
Breast reduction surgery can be performed at any age. It is, however, best performed after the breasts have matured. Breast reduction surgery can impair the ability to lactate ( breastfeed ). In case you are planning a future pregnancy, this must be brought to attention. The results of breast reduction can be affected by any future weight changes and pregnancy.
What are the steps involved in undergoing breast reduction surgery?
These are:
Preoperative consultation. You should be able to discuss your goals and expectations. We will be able to possible outcomes based on the physical examination findings. You must be prepared to the reveal history of any coexisting medical illness, medications, herbal supplements, any prior breast surgery. The incisions and scars location will be shown to you. The risks and possible complications are discussed. A mammogram is usually taken and depending on the findings further investigations like ultrasound may be ordered. Medical tests for fitness to undergo the procedure are obtained. Preoperative pictures are taken. You should feel free to clarify your doubts about the procedure.
Procedure. Breast reduction is usually carried out under general anesthesia. The incisions depend on the physical examination findings. They are usually,
- Around the areola
- Key hole shaped with the limb extending towards the fold on the undersurface of the breast.
- Inverted T-shaped with the horizontal limb under the breast.
The incisions are deepened after removal of excess skin. The breast tissues are reshaped and excess tissue is removed. Sutures are placed to hold the breast tissue together and incisions are closed with sutures and tapes. There may be thin tubes placed which help prevent accumulation of fluids at the operated site. Dressings comprise of soft pads placed in a surgical bra.
Recovery. Patients are encouraged to move about when they recover from anesthesia. The dressings are removed during the second day after surgery. The drains are removed depending upon the output. Patients are advised to cover the suture lines with dressing till suture removal. Most sutures are removed by the end of the first week and rest are removed at the end of the second week. A support bra has to be worn till three months. Light activities are permitted after the first week. Overhead movements of arms are restricted till the end of three weeks. It is usual to have swelling and some bruising at the operated site. These gradually resolve with time. Some patients may have numbness of skin near the scar. In most cases these settle without any intervention.
Will breast reduction impair the ability to lactate?
Yes, it can.
Will it affect imaging studies after surgery?
Yes. It can result in changes which can affect the interpretation of imaging studies on the breast.
What are the benefits of undergoing breast reduction?
These include,
- Improvement in self-esteem and confidence.
- Reduction in symptoms due to the physical effects like backache, maceration, indentation of skin etc.
- Improved contour and size proportionate to the body.
To learn more about secondary breast reduction, click here.
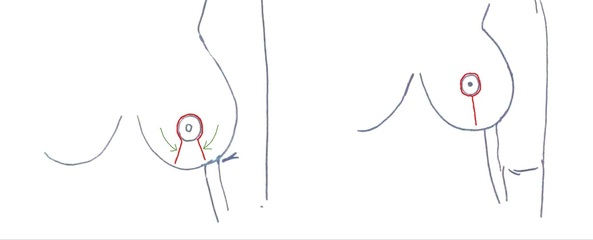
Breast reduction with key-hole incision. It extends from around the areola towards the inferior fold of breast.

Before breast reduction
|

After breast reduction (medial pedicle technique)
|
Breast reduction using medial pedicle technique. 500 gm and 600 gm were removed from the right and left breasts.

Before breast reduction (Frontal)
|

Before breast reduction (Lateral)
|

After breast reduction (at 10 days post-op)
|

After breast reduction (at one month post-op)
|

After breast reduction (at one month post-op)
|
Secondary breast reduction. First surgery was carried out elsewhere in 2014 (5 years back).

Before secondary breast reduction
|

After secondary breast reduction (2 months post-op)
|

Before: Macromastia with lipodystrophy
|

Preoperative marking
|

After: Appearance at 2 weeks
|

After: Appearance at 6 weeks. The swelling takes longer to subside
|

